Another piece of misleading science hasentered the SARS-CoV-2 (SC-2) variant debate: https://www.biorxiv.org/content/10.64898/2026.06.05.730251v2.full.
The authors of this recent paper on BA.3.2.2propose that the apparent enrichment of this highly mutated sublineage inpediatric populations could provide an immunological niche in which the virusmay continue to propagate, potentially catalyzing the emergence of secondary variantscapable of breaching the imprinted immunity of highly COVID-19 (C-19)-vaccinatedadult populations. They therefore suggest that future pediatric SC-2vaccination strategies should consider variant-matched antigens that combine ‘variant-matchedspecificity’ with ‘legacy-like breadth.’
This conclusion is not only the purestnonsense from a scientific standpoint; it rests on a fundamentalmisinterpretation of what the current BA.3.2.2 signal most likely represents.
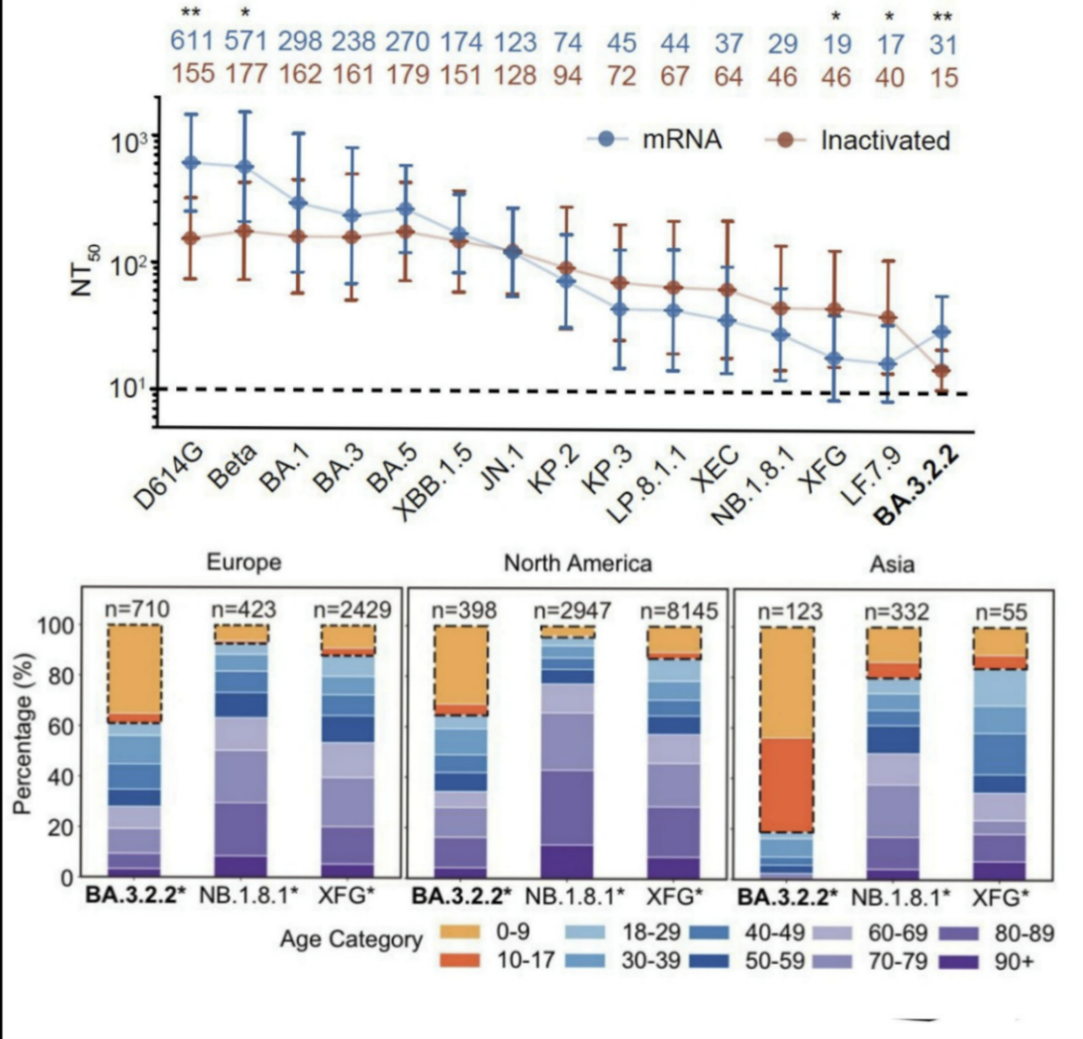
The increased representation of BA.3.2.2sequences in younger age groups may indeed be visible in some age-annotatedsequencing datasets (see below). However, this should not be confused withrobust evidence that BA.3.2.2 is infecting children more efficiently at thepopulation level, let alone that it has become evolutionarily adapted tochildren as a distinct biological niche.
Sequencing data are inherently conditioned by who gets tested, whose samplesare selected for sequencing, how outbreaks are investigated, and how completethe age metadata are. A pediatric enrichment signal in sequence datasets istherefore not equivalent to proof of sustained pediatric transmission.
Even if BA.3.2.2 were genuinelyoverrepresented among samples from young children, this would still not implythat children serve as a persistent reservoir for BA.3.2-derived sublineages.
It would at most indicate that this lineage is exploiting a transient,immune-history-dependent vulnerability in a demographic group whose immunelandscape differs from that of highly C-19-vaccinated adults.
The real issue is not pediatricsusceptibility. The real issue is the remarkable contribution of BA.3.2.2 tothe current SC-2 landscape as a direct consequence of the increasinglyconstrained nature of spike (S)-based immune escape from suboptimalpopulation-level immunity following the mass C-19 vaccination campaign.
BA.3.2-derived sublineages illustrate how theevolutionary bandwidth of SC-2 in highly C-19-vaccinated populations isbecoming increasingly constrained. As previously discussed in several of mymore recent substack articles (https://voiceforscienceandsolidarity.substack.com/), the virus continues to accumulate immune-escape mutations within the Sprotein, while each additional mutation appears to yield only diminishingreturns in terms of transmissibility.
In other words, a lineage can still moveantigenically, but the accessible beneficial moves become progressivelynarrower, more conditional, and more host-history-dependent.
This interpretation is fully compatible withthe authors’ observation that BA.3.2.2 shows an unusual relationship withimmune imprinting and antibody (Ab)-repertoire composition. They argue thatBA.3.2.2 preferentially escapes Omicron-specific Class 1/4 Abs enriched inweakly ancestral-imprinted individuals, while remaining sensitive toWuhan-cross-reactive IGHV3-53/66-encoded Class 1 Abs enriched in stronglyimprinted individuals. But this does not prove that BA.3.2.2 ischild-adapted. It merely shows that the lineage may exploit a particular Ab-repertoireconfiguration.
The authors point out that a comparable ageskew was not observed during the major antigenic transition from XBB-lineageviruses to BA.2.86/JN.1, despite the broad humoral immune escape and antigenicdistinctiveness of the latter lineage. In their view, this contrast arguesagainst immunological naivety alone as the primary driver of BA.3.2.2enrichment in children. It is therefore important to consider that theXBB-to-BA.2.86/JN.1 transition was largely driven by escape from broadlyneutralizing Ab activity, whereas BA.3.2.2 reflects a more constrainedand conditional form of S adaptation. Through incremental,threshold-reaching accumulation of S mutations, BA.3.2.2 may not only escapeOmicron-refocused Class 1/4 Abs in weakly ancestral-imprinted hosts, but mayalso partially remodel conserved infection-inhibiting RBD epitopes normallytargeted by broadly reactive, naturally occurring IgM Abs in young children.
If so, this could explain why children maybe transiently more susceptible to BA.3.2.2 than to BA.2.86/JN.1. However, suchsusceptibility would not imply genuine pediatric adaptation or durablechild-driven transmission.
Rather, it would reflect a temporary breachof a broadly reactive innate-Ab barrier and a conditional,immune-history-dependent advantage in hosts whose Ab repertoire is dominated bybroadly RBD-binding, cross-reactive but weakly neutralizing Omicron-refocusedspecificities. However, this window would be expected to close rapidly asinnate immune training intensifies in the pediatric cohort, thereby turningchildren from a temporarily permissive segment into an increasingly resistantbarrier to sustained BA.3.2.2 transmission.
This is because children are not to be considered miniature adults! Theirimmune protection against SC-2 is not primarily shaped by the samevaccine-imprinted, repeatedly recalled, antigen-specific adaptive immunepathways that dominate in highly C-19-vaccinated adult populations.
Young children rely far more heavily on broadly reactive innate immunemechanisms and natural Abs. Upon repeated exposure to highly transmissible SC-2variants, these innate immune mechanisms, including their cell-mediated innateimmune responses, can be rapidly and efficiently trained.
This is precisely why the idea of childrenserving as a persistent reservoir for BA.3.2.2 is immunologically implausible. A temporarily more susceptible pediatric segment will quickly andefficiently develop sterilizing immunity. In the presence of circulatingvirus, young children are repeatedly exposed to circulating SC-2 variants andthis progressively trains broadly protective innate immune responses. As thisprocess unfolds, the pool of truly susceptible pediatric hosts rapidly contractsrather than expands.
This is not the first time that a temporary pediatric signal has been misreadas evidence of a unique pediatric disease or transmission niche. We saw similarreasoning during the MIS-C (Multisystem Inflammatory Syndrome in Children) episode,when increased disease burden in children was widely interpreted as evidence ofa distinct child-specific pathogenic phenomenon. Yet those patterns wanedwithout requiring mass pediatric C-19 vaccination. The more plausibleexplanation was maturation and training of broadly protective immune responsesin successive pediatric cohorts. But not a single one of the so-called experts or public healthauthorities admitted that they had completely missed the ball in persuadingparents to let their young children get vaccinated!
It is reasonable to assume that a similarlogic applies here.
Temporarily enhanced prevalence of BA.3.2.2 inyounger age groups does not establish children as a reservoir. It more likelyreflects the fact that young children occupy a different immunologicallandscape from highly C-19-vaccinated adults.
This reverses the authors’ interpretation: the problem does not lie withthe pediatric population. The problem lies with the mass C-19 vaccination experiment,which generated the suboptimal, vaccine-imprinted population-level immunelandscape now shaping SC-2 evolution.
The authors’ proposal to vaccinate childrenwith C-19 vaccines that combine variant-matched specificity with legacy-likebreadth therefore completely misses the point.
Such a strategy would not solve the problem; it would risk dragging childreninto the same vaccine-imprinted immune landscape that is already drivingconstrained S-based immune escape in adults.
Young, unvaccinated children are precisely thepopulation segment in which broadly reactive innate immune training can stilloccur rapidly and efficiently. This process can provide protection againsthighly mutated sublineages such as BA.3.2.2 and may even generate sterilizingimmunity in the pediatric cohort.
Instead of acting as a durable reservoir for BA.3.2.2, children aretherefore more likely to become an increasingly resistant barrier to sustainedtransmission.
This is why the narrative of sustainedBA.3.2.2 transmission in pediatric populations ─ allegedly catalyzing theemergence of secondary variants that combine pediatric-evading features withadult-evading mutations and thereby allow the lineage to breach adult imprintedimmunity ─ will likely prove to be yet another myth.
The more plausible scenario is the opposite:
As pediatric populations develop sterilizingimmunity through rapid innate immune training, they will exert additional,non-selective immune pressure on viral transmissibility.
This pressure will no longer primarily favor incremental antigenic escapewithin S. Rather, it may help pave the way toward a major viral phasetransition.
In my framework, that transition would,therefore, not be mediated by yet another round of classical epitope-specificimmune escape. It would be mediated by non-antigen-specific,infection-enhancing changes, including mutations affecting glycosylationpatterns or glycan-dependent interactions. These are the kinds ofchanges I have postulated for Hi-Vi-Cron: a coronavirus phenotype capable ofsubverting suboptimal adaptive immunity in highly C-19-vaccinated populationsand thereby breaching the massive vaccine-imprinted immune barrier.
In conclusion, BA.3.2.2 does not reveal atruly child-adapted phenotype. It exposes a repertoire-dependent vulnerabilityin weakly ancestral-imprinted hosts. The pediatric enrichment signal should notbe mistaken for evidence of a durable child reservoir, nor should it be abusedto justify yet another pediatric C-19 vaccination campaign!
The authors’ conclusion turns cause and effectupside down. Children are not the problem. Theimmunological landscape created by the insane mass C-19 vaccination experiment isthe problem.
BA.3.2.2 is not a warning that children must be vaccinated. It is awarning that SC-2 is running out of productive S-based escape options within ahighly C-19-vaccine-imprinted population, and that the nextevolutionary step may no longer look like ordinary antigenic drift.

Geert Vanden Bossche received his DVM from the University of Ghent, Belgium, and his PhD degree in Virology from the University of Hohenheim, Germany. He held adjunct faculty appointments at universities in Belgium and Germany. After his career in Academia, Geert joined several vaccine companies (GSK Biologicals, Novartis Vaccines, Solvay Biologicals) to serve various roles in vaccine R&D as well as in late vaccine development.
Geert then moved on to join the Bill & Melinda Gates Foundation’s Global Health Discovery team in Seattle (USA) as Senior Program Officer; he then worked with the Global Alliance for Vaccines and Immunization (GAVI) in Geneva as Senior Ebola Program Manager. At GAVI he tracked efforts to develop an Ebola vaccine. He also represented GAVI in fora with other partners, including WHO, to review progress on the fight against Ebola and to build plans for global pandemic preparedness.
Back in 2015, Geert scrutinized and questioned the safety of the Ebola vaccine that was used in ring vaccination trials conducted by WHO in Guinea. His critical scientific analysis and report on the data published by WHO in the Lancet in 2015 was sent to all international health and regulatory authorities involved in the Ebola vaccination program. After working for GAVI, Geert joined the German Center for Infection Research in Cologne as Head of the Vaccine Development Office. He is at present primarily serving as a Biotech / Vaccine consultant while also conducting his own research on Natural Killer cell-based vaccines.
Email: info@voiceforscienceandsolidarity.org


.jpg)