Author: G. Vanden Bossche June 15th, 2026
BA.3.2.2 and theImaginary Child Reservoir: How a Sequencing Signal Becomes an insaneVaccination Sales Pitch
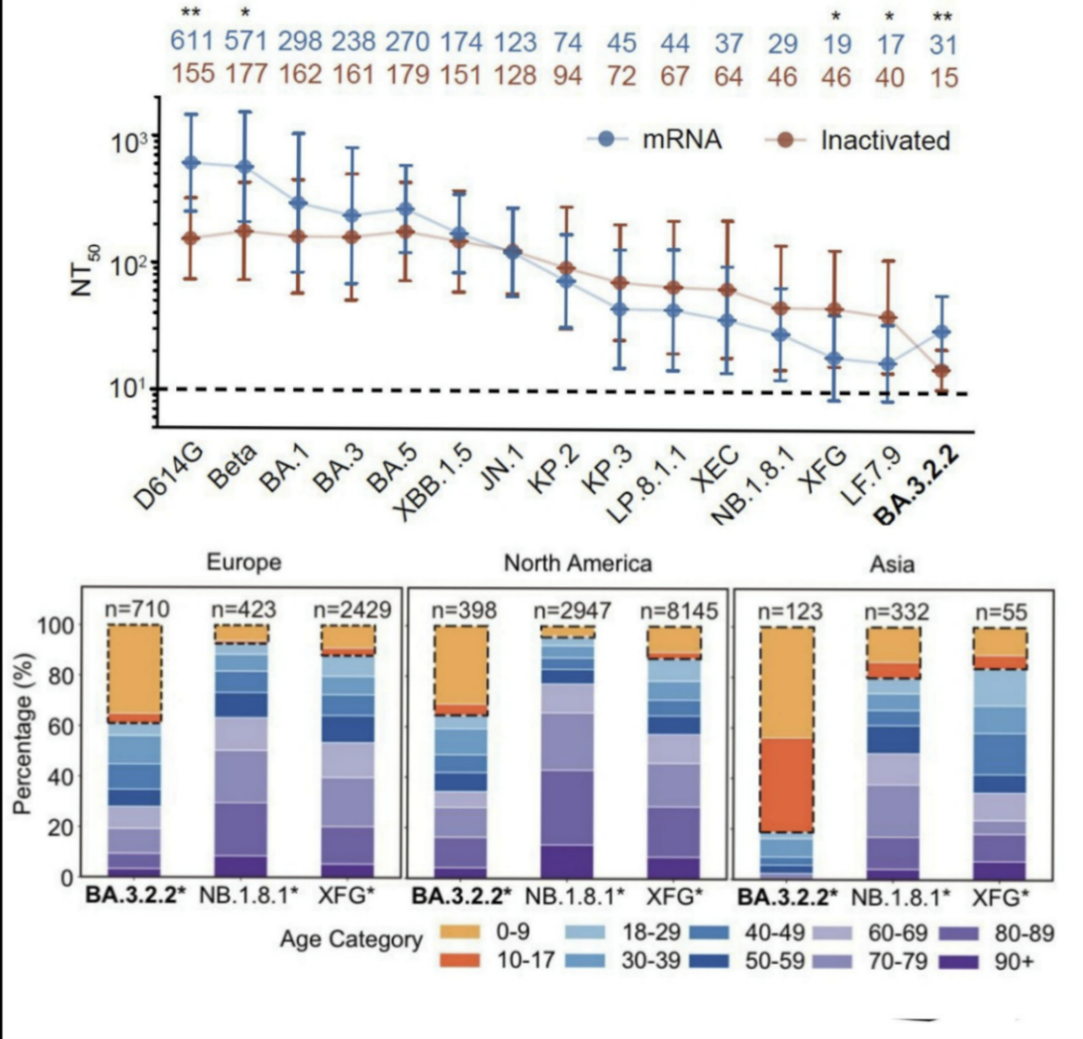
A newscientific paper suggests that the SARS-CoV-2 (SC-2) sublineage BA.3.2.2 may bespreading more easily in children and that children could become a reservoirfrom which new variants might emerge (https://www.biorxiv.org/content/10.64898/2026.06.05.730251v2.full).
The authors even suggest that this could justify future COVID-19 (C-19) vaccinationcampaigns in children using updated, variant-matched vaccines.
This interpretation is deeply misleading.
The first problem is simple: finding moreBA.3.2.2 sequences in children (see below) does not automatically mean thatthis variant is truly better adapted to children. Sequencing data are not thesame as real-world infection rates. They depend on who gets tested, whosesamples are selected for sequencing, where outbreaks are investigated andwhether age information is properly recorded. So, even if BA.3.2.2 appears moreoften in samples from children, this does not prove that children are a specialreservoir for this virus.
But even if BA.3.2.2 were temporarily morecommon in children, that still would not mean that the virus has become‘child-adapted.’
A much more plausible explanation is that children simply have a differentimmune background from highly C-19-vaccinated adults. Most adults in highly C-19-vaccinatedcountries have been repeatedly exposed to the spike (S) protein throughvaccination and vaccine-breakthrough infections. Their immune systems havetherefore been strongly shaped by repeated exposure to SC-2 antigens. This hascreated a highly complex, vaccine-imprinted immune landscape. The virus is nowtrying to escape from this population-level immune pressure, but it is becomingincreasingly constrained.
BA.3.2-derived sublineages illustrate this very well. As previously discussedin several of my more recent substack articles (https://voiceforscienceandsolidarity.substack.com/), the virus can still add new mutations in the S protein but eachadditional mutation seems to provide only a smaller and more conditionaladvantage.
In other words, the virus can still move, but it has less and less room tomove. Its evolutionary options are becoming narrower.
This is why BA.3.2.2 should not be seenas evidence of a new child-specific viral strategy. It is more likely asign that SC-2 is running into the limits of classical S-based immune escape inhighly C-19-vaccinated populations.
The authors argue that children, especiallythose without strong exposure to the original Wuhan-like virus or original C-19vaccines, may provide a special immunological niche for BA.3.2.2. Butthis turns the situation upside down.
Children are not just small adults. Their immune systems workdifferently. Young children rely more strongly on broad, fast-reactinginnate humoral and cellular immune effectors. These effectors are notnarrowly directed against one specific S variant. They can be trained rapidlythrough natural exposure to circulating respiratory viruses, including SC-2.
Theauthors also note that a similar age pattern was not seen when the virus movedfrom XBB-lineage variants to BA.2.86/JN.1, even though BA.2.86/JN.1 was alsoantigenically distinct and escaped many antibodies (Abs). They argue that thismeans simple immune naivety cannot fully explain why BA.3.2.2 appears moreoften in children. That point deserves an answer.
Inmy view, the XBB-to-BA.2.86/JN.1 transition was mainly about escape fromstrong, broadly neutralizing Abs. BA.3.2.2 seems different. It may represent amore limited and stepwise form of S adaptation. By accumulating enough Smutations, BA.3.2.2 may escape not only Omicron-refocused Abs in weaklyimprinted people, but also partly alter conserved RBD regions that are normallyrecognized by broad, naturally occurring IgM Abs in young children. These IgM Absare part of the child's early, innate-like defense against infection.
Ifthat is correct, children could be temporarily more susceptible to BA.3.2.2than to BA.2.86/JN.1. But this would still not mean that BA.3.2.2 is trulyadapted to children or that children will become a lasting reservoir.
It would only mean that the virus has found a short-lived opening in a broadinnate-Ab barrier. That opening should close rapidly as children's innateimmune responses are trained by exposure, turning children from a temporarilypermissive group into an increasingly resistant barrier to sustained BA.3.2.2transmission.
This is important. A child who is immunologicallynaïve and more susceptible today can quickly and efficiently train its innateimmune system as it gets exposed to circulating SC-2 variants. As this happens,the pool of truly susceptible children shrinks. Instead of becoming apermanent reservoir for BA.3.2.2, children are likely to become increasinglyresistant to this and other co-circulating variants.
We saw a similar mistake during the MIS-C (MultisystemInflammatory Syndrome in Children). At the time, some interpreted the increaseddisease burden in children as evidence of a special pediatric problem thatrequired mass C-19 vaccination of children!
But the pattern faded. A more plausible explanation is that children’s immunesystems matured and became broadly trained through exposure. But not a singleone of the so-called experts or public health authorities admitted that theyhad completely missed the ball in persuading parents to let their youngchildren get vaccinated!
It is reasonable to assume that a similar logic applies here. A temporaryincrease of BA.3.2.2 in children does not prove sustained child-driventransmission! It simply reflects a temporary gap in immune experience. Thatgap will close naturally as children get repeatedly exposed and develop broadnatural immune protection.
The authors’ suggestion that children shouldbe vaccinated with updated C-19 vaccines therefore misses the point.
If the current problem is the result of a C-19-vaccine-imprinted immunelandscape in adults, then imposing a similar vaccine imprint on children is nota solution. It may simply drag children into the same immunological trap.
Young, unvaccinated children may still be ableto develop broad, naturally trained protection against SC-2. This protectionis not based on repeatedly chasing the latest S variant with updated C-19 vaccines.It is based on the rapid training of innate immune defenses, whichreduce infection, viral replication, and transmission.
This is why children will not serve as a persistent reservoir forBA.3.2.2. This is also why BA.3.2.2 is not going to maintain itselfindefinitely by spreading through children.
The more likely outcome is that children will become increasingly resistant,thereby adding further non-selective immune pressure on the virus.
This additional pressure may have an importantconsequence, though. It may not simply push the virus toward yet another smallstep in S-based immune escape. Instead, it may push the virus toward amore dramatic evolutionary transition.
In my view, SC-2 is now approaching the limitsof ordinary antigenic drift. The virus may therefore be forced to find adifferent route to increase its fitness. I strongly believe that this route willinvolve changes that are not primarily directed at escaping specific Abepitopes but at enhancing systemic infection through other mechanisms,such as altered glycosylation patterns or glycan-dependent interactions.This is the type of transition I have described in relation to Hi-Vi-Cron.
In that scenario, the real danger is not thatchildren will become a permanent reservoir for BA.3.2.2. The real danger isthat the virus, under growing immune pressure from C-19 vaccinated adults andincreasingly resistant children, may be pushed toward a major phase transition.
That is why the current pediatric BA.3.2.2narrative is so misleading. It takes a sequencing signal and turns it into avaccine argument. It suggests that children are the problem, when in realitythe problem is the population-level immune landscape created by the mass C-19vaccination experiment.
BA.3.2.2 is, therefore, not a warning thatchildren need another C-19 vaccine. It is a warning that SC-2 is running out ofproductive S-based escape options in highly C-19-vaccinated populations. Children are not the reservoir. Children are more likely to become thebarrier.
And that is exactly why the proposal to vaccinate them against this supposedpediatric threat is not only unnecessary, but immunologically insane.

Geert Vanden Bossche received his DVM from the University of Ghent, Belgium, and his PhD degree in Virology from the University of Hohenheim, Germany. He held adjunct faculty appointments at universities in Belgium and Germany. After his career in Academia, Geert joined several vaccine companies (GSK Biologicals, Novartis Vaccines, Solvay Biologicals) to serve various roles in vaccine R&D as well as in late vaccine development.
Geert then moved on to join the Bill & Melinda Gates Foundation’s Global Health Discovery team in Seattle (USA) as Senior Program Officer; he then worked with the Global Alliance for Vaccines and Immunization (GAVI) in Geneva as Senior Ebola Program Manager. At GAVI he tracked efforts to develop an Ebola vaccine. He also represented GAVI in fora with other partners, including WHO, to review progress on the fight against Ebola and to build plans for global pandemic preparedness.
Back in 2015, Geert scrutinized and questioned the safety of the Ebola vaccine that was used in ring vaccination trials conducted by WHO in Guinea. His critical scientific analysis and report on the data published by WHO in the Lancet in 2015 was sent to all international health and regulatory authorities involved in the Ebola vaccination program. After working for GAVI, Geert joined the German Center for Infection Research in Cologne as Head of the Vaccine Development Office. He is at present primarily serving as a Biotech / Vaccine consultant while also conducting his own research on Natural Killer cell-based vaccines.
Email: info@voiceforscienceandsolidarity.org


.jpg)